DOES THE SIZE OF THE BALL MATTER IN THR
The size of the ball of the natural hip joint (femoral head) varies and usually ranges from 40 to 54 mm (with smaller sizes in females). During the initial development of hip replacement, the surgeons tried to make the implants which mimic the size of the natural femoral head. However, it was soon realised that when a large metal ball articulates with a plastic cup, the plastic part gets worn out quickly due to “volumetric wear”. To decrease the “wear” of the plastic, Sir John Charnley (who was one of the pioneers in the development of modern hip replacements), opted for a smaller 22 mm metal head (which is much smaller than the natural femoral head) in the design of Charnley hip replacement. This design was the commonest hip replacement done in the UK until recently.
Studies have shown that with this technique, there were fairly good long term results in patients who are not very young and active. However, there were some restrictions placed on what the patients can do to avoid dislocations (when the ball comes out of the joint) and a high dislocation rate following hip replacement has been quoted with smaller “ball size” in multicentre studies1.
Many surgeons over the past few years have started using slightly larger size femoral head (28 mm) which is still within the tolerance of conventional metal on plastic bearing. However, still it is smaller than the natural femoral head. The problem of wear and dislocation is still a potential concern.
Dislocation still remains a major reason (17%) for revision of hip replacement (NJR data 2008).

A study2 in which Mr.Ganapathi was involved found that the financial cost of treating dislocated hip replacements was high (£500000 on a conservative estimate in dealing with 100 first time dislocators). In addition many patients had to undergo further revision surgeries and the functional results were less than optimal. While the cause of hip dislocations is multifactorial, using a larger ball could decrease the incident of dislocations. However, the size of the ball was limited by the material properties.
In addition, much younger and active patients are being offered hip replacements now. The expectations of young and active patients are much higher and they would like to go back to their active lifestyle with little restrictions. To improve the durability of the hip replacements, material scientists have come up with modern solutions (alternative bearings).
There are essentially three types of alternative materials – cross linked poly (plastic), ceramic and metal. These alternative bearings also allow larger size ball to be used 32 mm, 36 mm and even 40 mm. However, the size would be limited by the cup (socket size) and also some material allow slightly bigger ball to be used with the same cup size compared to other materials.


Stability +
ROM +
Bone conserving –
(ROM –


Stability ++
ROM ++
Bone conserving –


Stability +++
ROM ++
Bone conserving +


Stability +++
ROM +++
Bone conserving –
Lab studies and clinical studies also support the concept that the larger sized balls decrease the dislocation3,4. A study conducted by Mr.Ganapathi also found that the larger size ball also decrease the risk of dislocations even in complex revision surgery compared with historical studies5.
However, because of the relatively new concept, the “modern” alternative bearings brought some new complications. Metal on metal bearings, in addition also allowed the surgeon to use an even larger size ball (same size as the natural femoral head – “anatomical sized head” or “large diameter head”). Because the size of the ball is almost the same as the natural femoral head, there is almost a negligible rate of dislocation and very little restriction in activities once the soft tissues have healed. Data from some studies on gait analysis showed better gait pattern with larger diameter balls 6,7 and better patient reported outcome scores8.
A study from Montreal9 in which Mr.Ganapathi was involved analysed the range of movement following different types of hip replacement using standardised digital photographs and computer software.
This study showed that the range of movement was better with the “large diameter head” total hip arthroplasty when compared with 28 mm head total hip arthroplasty or hip resurfacing but still was less than the range of movement of the normal contralateral hip. In addition, functional score (WOMAC score) also correlated with range of movement.

This study showed that the range of movement was better with the “large diameter head” total hip arthroplasty when compared with 28 mm head total hip arthroplasty or hip resurfacing but still was less than the range of movement of the normal contralateral hip. In addition, functional score (WOMAC score) also correlated with range of movement.
Examples of stability and range of movement achieved Following hip replacement using large diameter head
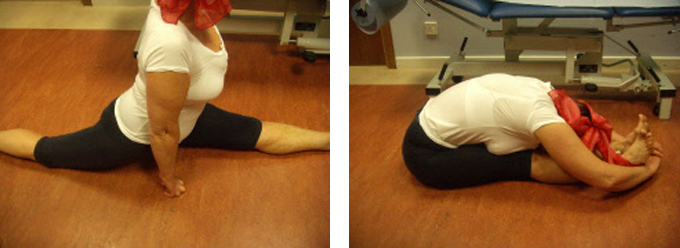
1. Yoga teacher –
2. Skiing Instructor – 4 months following large diameter head and hip replacement
Although, large head metal on metal type hip replacements/hip resurfacing appeared to be the ideal bearing option with regards to stability and range of movement, further studies indicated higher early failure rate with metal on metal hip replacements and hip resurfacing. In April 2010 MHRA (Medicines and Healthcare products Regulatory Authority) issued an alert to the higher failure rate. In April 2010 MHRA (Medicines and Healthcare products Regulatory Authority) issued an alert to the high failure rate of metal on metal hips and advised monitoring of patients with metal on metal hips with metal ion levels in the blood.
Over the ensuing few years, metal on metal bearings including resurfacings gradually fell out of favour and is done very infrequently. Currently, the most common bearing options used are metal on cross linked plastic, ceramic on cross linked and ceramic and ceramic bearings with still some limitations.
Thus the quest for the optimal bearing surface still continues!
Current view: Although anatomical size balls had many theoretical and practical advantages including excellent hip stability compared to traditional smaller balls, the higher complications and higher revision rate with metal on metal large head hip replacements and hip resurfacings have led to a general trend of avoiding very large balls and such large ball metal on metal bearings are very rarely used nowadays. As a compromise between stability, range of movement and avoidance of complications of anatomical sized metal on metal bearings, medium sized 32 mm or 36 mm balls are being increasingly used.
Scientific Literature
The following are some relevant selected scientific references:
1. Outcome of Charnley total hip replacement across a single health region in England: the results at five years from a regional hip register.
J Bone Joint Surg Br. 1999 Jul;81(4):577-
Fender D, Harper WM, Gregg PJ.
Using a regional arthroplasty register we assessed the outcome at five years of 1198 primary Charnley total hip replacements (THRs) carried out in 1152 patients across a single UK health region in 1990. Information regarding outcome was available for 1080 hips (90%) and 499 had an independent clinical and radiological assessment. By five years the known rate of aseptic loosening was 2.3%, of deep infection 1.4%, of dislocation 5.0% and of revision 3.2%. The radiological assessment of 499 THRs revealed gross failure in a further 5.2%, which had been previously unrecognised. The combined rate of failure of nearly 9% is higher than those published from specialist centres and surgeons, but is probably more representative of the norm. Our study supports the need for a national register and surveillance of THRs. It emphasises that all implants should be followed, and suggests that the results of such surgery, when performed in the general setting, may not be as good as expected.
2. Outcome of treatment for dislocation after primary total hip replacement.
J Bone Joint Surg Br. 2009 Mar;91(3):321-
Kotwal RS, Ganapathi M, John A, Maheson M, Jones SA.
We have studied the natural history of a first episode of dislocation after primary total hip replacement (THR) to clarify the incidence of recurrent dislocation, the need for subsequent revision and the quality of life of these patients. Over a six-
3. A cadaveric study of posterior dislocation after total hip replacement-
Int Orthop. 2010 Feb 24. [Epub ahead of print].
Ng FY, Zhang JT, Chiu KY, Yan CH.
The size of the femoral head and acetabular anteversion are crucial for stability in total hip replacements. This study examined the effects of head diameter and acetabular anteversion on the posterior instability after total hip replacement in an in vivo setting. The acetabular shell was inserted at 0-
4. Hip stability in primary total hip arthroplasty using an anatomically sized femoral head.
Orthopedics. 2009 Jul;32(7):489. Smit MJ.
Dislocation after total hip arthroplasty (THA) remains a problem despite many advances in technique and prosthetic design over the 5 decades since the introduction of total joint replacement. This article reports the short-
5. The use of large diameter femoral heads in revision total hip replacement
Journal of Bone and Joint Surgery –
M Ganapathi; I B Paul; E Clatworthy; A John; M Maheson; and S Jones
Aim: To investigate the outcome following revision total hip arthroplasty (THA) using 36 mm and 40 mm modular femoral heads. Methods: Details were retrieved from our arthroplasty database regarding all revision THAs done in our unit using 36 mm and 40 mm femoral heads. Follow-
6. Postural balance during quiet standing in patients with total hip arthroplasty and surface replacement arthroplasty.
Clin Biomech (Bristol, Avon). 2008 May;23(4):402-
Nantel J, Termoz N, Centomo H, Lavigne M, Vendittoli PA, Prince F.
BACKGROUND: Primary total hip arthroplasty leads to better functional capacities but a general weakness of abductor muscles often persists. A larger head component may improve the postural balance in the medial-
7. Postural balance during quiet standing in patients with total hip arthroplasty with large diameter femoral head and surface replacement arthroplasty.
rch Phys Med Rehabil. 2009 Sep;90(9):1607-
Nantel J, Termoz N, Ganapathi M, Vendittoli PA, Lavigne M, Prince F.
OBJECTIVE: To compare postural balance between patients who have had either a large diameter head total hip arthroplasty or surface replacement arthroplasty. DESIGN: Observational study. SETTING: Outpatient biomechanical laboratory. PARTICIPANTS: Two groups of 14 patients with surface replacement or large diameter head total hip arthroplasties recruited from a larger randomized study and 14 control subjects. INTERVENTIONS: Not applicable. MAIN OUTCOME MEASURES: Postural balance during quiet standing in dual and one-
8. Comparison of patient-
J Bone Joint Surg Br. 2009 Dec;91(12):1550-
Department of Orthopaedics, Freeman Hospital, High Heaton, Newcastle upon Tyne, UK.
This study compared the demographic, clinical and patient-
9. Range of motion of large head total hip arthroplasty is greater than 28 mm total hip arthroplasty or hip resurfacing.
Accepted for publication in Clin Biomech.
Lavigne M, Ganapathi M, Mottard S, Girard J, Vendittoli P.
Department of Surgery, Maisonneuve-
Background: Reduced range of motion of the hip has a detrimental influence on lower limb function. Large diameter head total hip arthroplasty may theoretically have a greater potential for restoring normal hip range of motion due to greater head-
Method: At minimum one year follow-
Findings: The large diameter head total hip arthroplasty group had significantly greater total arcs of motion (approximately 20 degrees), mostly due to an increase of hip flexion and external rotation, but did not reach normal hip motion. The hip range of motion showed significant correlation with the WOMAC score, especially the flexion arc.
Interpretation: The better hip range of motion of large diameter head total hip arthroplasty is likely due to the greater head to neck diameter ratio and hence seems to be the best option to optimize range of hip motion and improve function after hip arthroplasty.