PARTIAL KNEE REPLACEMENT
In these type of knee replacements only part of the knee is replaced unlike a total knee replacement. There are essentially two types of partial knee replacements – unicompartmental knee replacement and patellofemoral replacement.
Unicompartmental Knee replacement:
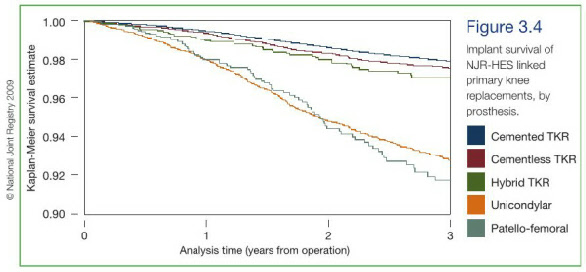
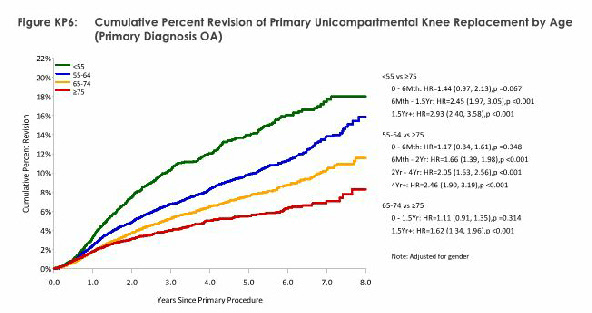
Knee arthritis often starts in the inner aspect of the knee (medial compartment) and affects other parts later. In some patients with isolated medial compartment arthritis it may be appropriate to consider partial knee replacement of the inner compartment of the knee instead of a total knee replacement. The advantage of partial knee replacement is that the operation is done through a smaller incision (minimally invasive technique) and the recovery period is quicker. Only part of the knee which is affected is replaced. In addition, if the other parts of the knee joint become arthritic or symptomatic, a revision to a total knee replacement could be done. While good results have been reported by some studies, there are other studies (including national joint registries) have shown that the failure rate following unicompartmental knee replacement is somewhat higher than total knee replacement and other parts of the knee may become symptomatic requiring further revision surgery. Hence patient selection criteria is important and if you suitable for partial knee replacement Mr.Ganapathi would discuss the options with you.


Patello-
In some patients, the arthritis affects mainly the knee cap and other parts of the knee are not affected. The pain will mainly be in the front of the knee and gets worse with activities including climbing stairs (particularly downhill), walking uphill and downhill, getting up from a sitting posture and activities which involve bending of the knee. There may be also a sensation of catching of the knee/ giving away of the knee. In these situations, it would be possible to replace only the knee cap instead of a total knee replacement. The advantage is that the operation is of lesser magnitude, recovery is quicker and only the affected part is replaced. However, other parts of the knee may be affected at a later stage and may need further revision surgery to a total knee replacement. This type of replacement also has somewhat higher failure rate. If you are a suitable candidate Mr.Ganapathi would discuss the options with you.


The following are some relevant selected scientific references:
1. UK Joint Registry Data 2009-

2. UK Joint Registry Data 2009-
3. Australian Joint Registry Data 2009-

4. New Zealand Joint Registry Data 2008-
arthroplasty
5. Unicompartmental knee arthroplasty in patients aged less than 65.
Acta Orthop. 2010 Feb;81(1):90-
W-
Department of Orthopaedics, Clinical Sciences Lund, Lund University Hospital, Sweden.
Abstract:INTRODUCTION AND PURPOSE: In recent years, there has been renewed interest in using unicompartmental knee arthroplasty (UKA). Several studies have reported increasing numbers of UKAs for osteoarthritis in patients who are less than 65 years of age, with low revision rates. To describe and compare the use and outcome of UKA in this age group, we have combined data from the Australian and Swedish knee registries.
PATIENTS AND METHODS: More than 34,000 UKA procedures carried out between 1998 and 2007 were analyzed, and we focused on over 16,000 patients younger than 65 years to determine usage and to determine differences in the revision rate. Survival analysis was used to determine outcomes of revision related to age and sex, using any reason for revision as the endpoint.
RESULTS: Both countries showed a decreasing use of UKA in recent years in terms of the proportion of knee replacements and absolute numbers undertaken per year. The 7-
INTERPRETATION: The results of the combined UKA data from the Australian and Swedish registries show a uniformity of outcome between countries with patients aged less than 65 having a higher rate of revision than patients who were 65 or older. Surgeons and patients should be aware of the higher risk of revision in this age group.
6. Unicompartmental knee arthroplasty compares favorably to total knee arthroplasty in the same patient.
Orthopedics. 2009 Apr;32(4).
Dalury DF, Fisher DA, Adams MJ, Gonzales RA.
Department of Orthopedic Surgery, St Joseph Medical Center, Baltimore, Maryland, USA.
Abstract:There are several surgical management options for medial knee arthritis, and it is often difficult to decide whether a unicompartmental knee arthroplasty (UKA) or total knee arthroplasty (TKA) is appropriate. Few studies have compared UKAs and TKAs in the same patient. We identified 23 patients with osteoarthritis who had a TKA on one side and a UKA on the other. The preoperative values of the 2 knees were not statistically different. Strict criteria were used to determine whether a UKA could be performed (functional anterior cruciate ligament, minimal deformity, and minimum changes in other compartments). Preoperative radiographs were reviewed to confirm that the knee undergoing TKA had medial compartment disease only. Knee Society scores, radiographic analysis, and patient preferences were recorded for all patients. Average follow-
7. Unicompartmental knee replacements with Miller-
Int Orthop. 2010 Apr 25. [Epub ahead of print]
John J, Mauffrey C, May P.
Department of Trauma and Orthopaedics, Royal Derby Hospital, Derby City, UK.
Abstract: We report the outcome of 94 Miller-
8. Outcome of revision of unicompartmental knee replacement.
Acta Orthop. 2010 Feb;81(1):95-
Hang JR, Stanford TE, Graves SE, Davidson DC, de Steiger RN, Miller LN.
AOA National Joint Replacement Registry, University of Adelaide, SA, Australia.
Abstract: BACKGROUND AND PURPOSE: Despite concerns regarding a higher risk of revision, unicompartmental knee arthroplasty (UKA) continues to be used as an alternative to total knee arthroplasty (TKA). There are, however, limited data on the subsequent outcome when a UKA is revised. We examined the survivorship for primary UKA procedures that have been revised.
METHODS: We used data from the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) to analyze the survivorship of 1,948 revisions of primary UKA reported to the Registry between September 1999 and December 2008. This was compared to the results of revisions of primary TKA reported during the same period where both the femoral and tibial components were revised. The Kaplan-
RESULTS: When a primary UKA was revised to another UKA (both major and minor revisions), it had a cumulative per cent revision (CPR) of 28 and 30 at 3 years, respectively. The CPR at 3 years when a UKA was converted to a TKA was 10. This is similar to the 3-
INTERPRETATION: When a UKA requires revision, the best outcome is achieved when it is converted to a TKA. This procedure does, however, have a major risk of re-
9. Factors associated with reduced early survival in the Oxford phase III medial unicompartment knee replacement.
Knee. 2010 Jan;17(1):48-
Kuipers BM, Kollen BJ, Bots PC, Burger BJ, van Raay JJ, Tulp NJ, Verheyen CC.
Department of Orthopaedic Surgery, Isala Clinics, Zwolle, The Netherlands.
Abstract:The aim of this study was to determine the prognostic value of preoperative patellofemoral osteoarthritis, BMI and age for implant survival of unicompartmental knee arthroplasty (UKA) performed in patients meeting strict admission criteria. The data and radiographs of 437 unilateral Oxford phase III procedures (Biomet, Bridgend, UK) were analysed. All procedures were carried out or supervised by 13 specialised knee surgeons in three different hospitals. The study group comprised 437 patients with a median follow of 2.6 years (0.1-
10. Unicompartmental or total knee replacement: the 15-
J Bone Joint Surg Br. 2009 Jan;91(1):52-
Newman J, Pydisetty RV, Ackroyd C.
Avon Orthopaedic Centre, Southmead Hospital, Westbury-
Abstract: Between 1989 and 1992 we had 102 knees suitable for unicompartmental knee replacement (UKR). They were randomised to receive either a St Georg Sled UKR or a Kinematic modular total knee replacement (TKR). The early results demonstrated that the UKR group had less complications and more rapid rehabilitation than the TKR group. At five years there were an equal number of failures in the two groups but the UKR group had more excellent results and a greater range of movement. The cases were reviewed by a research nurse at 8, 10 and 12 years after operation. We report the outcome at 15 years follow-
10. The Oxford medial unicompartmental knee replacement using a minimally-
J Bone Joint Surg Br. 2006 Jan;88(1):54-
Pandit H, Jenkins C, Barker K, Dodd CA, Murray DW.
Department of Orthopaedic Surgery, Nuffield Orthopaedic Centre, Headington, Oxford OX3 7LD, UK.
Abstract: This prospective study describes the complications and survival of the first 688 Phase 3 Oxford medial unicompartmental knee replacements implanted using a minimally-