TOTAL HIP REPLACEMENT
TOTAL HIP REPLACEMENT
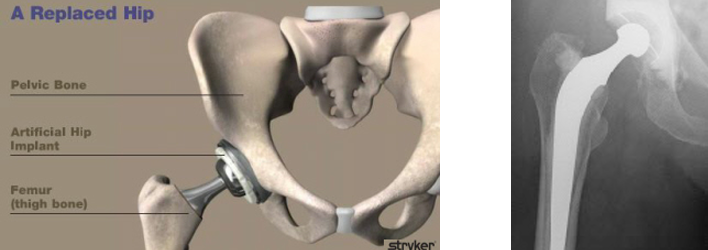
Hip joint is the joint between the thigh bone (femur) and the pelvis. The hip joint is a “ball and socket joint” similar to the shoulder joint allowing movements in all directions. While the main function of the shoulder is mobility, the hip has to be mobile as well as stable. So the hip joint is more congruous (the ball is seated deeper in the cup compared to the shoulder) and also supported by strong ligaments. The articulating parts are the femoral head (ball) and the acetabulum (socket). The articulating surfaces are covered with a special lining known as articular cartilage.

X-ray of a Normal Hip
Arthritis develops when the lining (articular cartilage) gets damaged due to various reasons including ‘wear and tear’ (osteoarthritis) as well as inflammatory conditions like rheumatoid arthritis. In addition arthritis in the hips can also develop secondary to a number of problems including mechanical problems like impingement syndrome, sequelae of child hood hip disorders like Perthe’s disease, problems with the blood supply (avascualr necrosis) as well as following trauma to the hip joint. The hip becomes painful. The initial management is non-

X-ray of an Arthritic Hip
When the pain due to knee arthritis increases and is not controlled by conservative measures, then it would be appropriate to consider surgical options which essentially means some form of hip replacement which would depend on the age and activity level of the patient.
Traditional Charnley hip replacement
Total hip replacement is considered to be one of the most successful operation of the 20th century. In this operation, the surgeon changes the ball and socket joint of the hip joint to an artificial joint. Sir John Charnley pioneered the development of hip replacement in the 1960’s. In the Charnley total hip replacement, both the acetabular component and the femoral component were cemented and the articular surface was a metal on plastic combination. The ball in the Charnley hip replacement is about 22 mm.
Since then more and more younger patients are being offered hip replacements and studies have shown that conventional hip replacements do not last long in young and active patients. In addition, the 22 mm ball also affords less stability of the hip replacement with risk of dislocation and dislocation rate of 5% has been quoted in studies.
With improvement in material science, further developments have been made to improve the longevity of the hip replacements particularly in young and active patients. Various implant devices have been introduced including different types of cemented devices and un-
In addition to the potential increased durability, the modern bearings also allow a bigger size ball to be used instead of the 22 mm ball used in Charnley total hip replacement. The bigger the ball of the hip replacement, the better the stability of the hip joint.
A study in which Mr.Ganapathi was involved found that over £500000 were spent (on a conservative estimate) in treating 100 patients with hip dislocations. In addition to the financial burden, the study also found that even after further revision surgery, the function and outcome score of the patients who had dislocation were inferior to those who did not have a dislocation. Recent studies have shown that the risk of dislocation could be reduced by larger size femoral head (ball of the hip joint). With the availability of modern material for bearing surfaces, it is possible to use a relatively larger ball than conventional total hip replacement (see does size matter?).
-

- X-rays of a patient with severe arthritis, shortening and deformity
-

- Post-operative x-rays after total hip replacement with uncemented hip replacement, ceramic bearing with 36 mm ball
Although, total hip replacement is a very successful procedure, like any major operation it has certain risks (although rare) including that of infection, bleeding, damage to the neurovascular structures, thrombo embolism (clots in the legs which can go to the lungs), dislocations, limb length discrepancy, periprosthetic fractures, anaesthetic complications etc., (see section on complication). The complication rate will be somewhat higher if the hip replacement is more complex (see revision hip replacement) and also when hip replacement is done for certain hip fractures. The complication rate to some extent will also depend on the individual patient’s medical status and Mr. Ganapathi will in some cases send you for an anaesthetic opinion before deciding on surgical treatment.
Complex total hip replacement ( some examples):
1. A relatively young patient with severe arthritis in the left hip with an almost fused hip (very stiff) with gross deformity, shortening and very abnormal gait.

Preoperative x-ray

Postoperative x-ray after hip replacement with a modular implant. Needed extensive soft tissue release to correct the deformity.
2. Fractures of the femoral neck (top of the thigh bone) are usually treated by internal fixation or hemiathroplasty (half hip replacement). However, recent evidence suggests that in some patients with displaced fracture of the neck of femur, a total hip replacement may give better function, although the complication rate like dislocation may be higher. The following is an example of a very unusual pattern of hip fracture treated with revision type hip replacement.
Frequently asked questions:
What type of anaesthesia will I have? The anaesthetist will discuss with you regarding the different types of anaesthesia (spinal or general). To decrease the postoperative pain, Mr. Ganapathi routinely injects the operated area with local anaesthetic which has been shown to decrease the use of painkillers which can make you drowsy.
How long will I stay in the hospital? The length of stay varies depending on the individual factors. Mr.Ganapathi emphasis on accelerated rehabilitation so that the patients regains optimal function soon. There is no minimum fixed time limit that you have stay in the hospital following hip replacement –
Will I have a minimally invasive hip replacement? Mr.Ganapathi also uses minimally invasive approach whenever suitable with a smaller incision than standard incision with less damage to the soft tissues. This is made possible by placing the incision in a slightly different place (more optimal place) than the standard incision and using special instruments. This allows good exposure of the hip joint even with a smaller incision.
What restriction will I have? Majority of patients who undergo hip replacement experience a dramatic reduction in the hip pain (groin pain) and improvement in functional activities. During the first 2-
What can I do in the long term? Like car tyres, the bearing surface of the hip joint also can wear with time and it would be appropriate to avoid high impact activities like jogging and high-
What can I do to optimize myself before surgery?
- Before the surgery, it is important that any medical problems (like high blood pressure, diabetes) which you may have are under control.
- If you are overweight, you should try to reduce the weight as studies have shown that the complication rates are somewhat higher in overweight patients undergoing hip replacement.
- Infection following a hip replacement is very rare. However, to decrease the risk of infection any foci of infection should be treated before surgery. If you have any skin infection it is important to have that treated before having a hip replacement. Similarly if there is water infection or dental infection this should be treated beforehand.
- Smoking increases the complications following major surgery. Cessation of smoking even for few weeks prior to surgery has been shown to decrease the complications.